Introduction
The demand for successful replacement of missing teeth with a functional and esthetic restoration that maintains the health of existing oral structures has significantly influenced prosthodontic treatment planning. The goal of prosthodontic treatment is to preserve and restore normal speech, masticatory function and provide aesthetic replacements on a long-term basis. Osseo-integrated dental implants have proven to be predictable for replacement of individual missing even though this treatment modality was originally introduced for completely edentulous patients[1]. Implant restorations predictably restore function, aesthetics, and phonetics.
Implant dentistry has made rapid and remarkable progress in recent years. Prosthetic reconstruction involving endosseous implants can be either screw-retained or cement-retained [2],[3]; however, controversial recommendations have been made regarding the type of retention of crown to abutment.[3],[4],[5],[6] The implant prosthesis may require removal for hygiene, repairs and abutment screw tightening[7]; and screw-retained prosthetic design made these procedures easy. Also, higher failure rates following implant placement necessitated frequent removal of the prosthesis.[8],[9],[10] Screw retention of implant-supported prostheses was validated by studies of the Branemark system.[8],[11],[12] With regard to single-tooth screw-retained restorations, Cordioli[13] and associates reported a total implant survival rate of 94.4%. Engquist and colleagues[14] reported a survival rate of 97.6% for single-tooth restorations.
Case Report
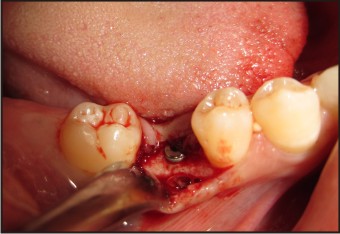
A 22 year old female reported to Government Dental College, Thiruvananthapuram for the replacement of her missing 46 (Fig 1). The patient was informed of the available treatment options. The tooth was extracted few years back due to caries and she wanted a fixed replacement for the tooth. A detailed medical and dental history was recorded and evaluated. Radiographs (panoramic radiograph and Intra oral Peri-apical radiograph) were used for assessment of the site of implantation. Patient education regarding the advantages, precautions, procedures, maintenance and post-operative care were given and an informed consent for the treatment by the patient and a witness was obtained. Routine blood analyses were done to assess the health status. Diagnostic cast were made and a surgical stent was fabricated using autopolymerising acrylic resin. The implant (ADIN IMPLANT SYSTEM, ISRAEL) of appropriate diameter and length was selected. The surgical procedure was done under antibiotic cover and sterilization protocol was strictly adhered to during the entire procedure.
 | Figure 1 : Pre-operative
 |
The area was anesthetised and an incision placed on the crest of the ridge to raise a flap. After marking the site using surgical stent, initial penetration through cortical bone was achieved with the use of 2.0 mm pilot drill. The largest drill size used depended on the diameter of the implant. Once the required depth was prepared, the implant was mounted on a carrier and was slowly driven to its final position using a wrench and cover screw was placed (Fig 2). Elevated flaps were approximated by interrupted sutures. A peri-apical radiograph was obtained to confirm the complete placement of the implants and to check its parallelism with adjacent teeth (Fig 3). Patient was given post-operative instructions. Suture removal was done after 7 days.
 | Figure 2 : Implant With Cover Screw
|
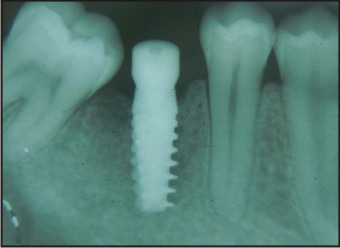 | Figure 3 : Post Surgical Iopa
|
The patient was recalled after 4 months for the second stage implant surgery. An incision was made to expose the cover screw which was then unscrewed in an anti-clockwise direction and removed. A healing abutment was then screwed into place. The flaps were approximated and sutured. After a period of 3 weeks, on removal of the healing abutment, a well formed gingival cuff was revealed around the implant. The implant impressions were made using a 2 mm thick custom tray fabricated using autopolymerizing acrylic resin with a window to allow space for the transfer coping secured to the implant fixture and impression made using multiple mix technique. Poly-vinyl siloxane impression material (ELITE HD DENTSPLY) of light body consistency was meticulously syringed all around the transfer coping. Poly-vinyl siloxane impression material (ELITE HD DENTSPLY) of regular body consistency was used to obtain the impression. After complete setting of the material, the custom tray was removed carefully from the patient’s mouth along with the transfer coping and disinfected. An implant analogue is positioned over the transfer coping and cast was poured. A plastic abutment was used for the fabrication of screw-retained implant crown. The final screw-retained single implant restoration was screwed into place with the application of 20 Ncm force (Fig 4). An intra-oral peri-apical radiograph was taken to ascertain the fit of the prostheses of the screw-retained. The screw access hole was filled using composite. After prosthetic phase, a follow-up program was designed for 6 months.
 | Figure 4 : A) Pre-operative B) Post-operative
|
Discussion
The replacement of a single missing tooth with a dental implant should not only restore function but also esthetics. The replaced teeth should create an illusion of a natural dentogingival complex, thus forming the appearance of intact natural tooth at the missing tooth site. The restoration must first fulfil the treatment goals that are crucial to the location of the missing tooth. Restoration of dental implants requires the involvement of both the restoring dentist and the dental technician to achieve a functionally and aesthetically pleasing result. From a clinical point of view, one of the factors affecting the long-term success of implant restorations is considered to be mechanical resistance of both the implant-prosthetic connection system and the restorative material itself[15],[16],[17].
Currently, there are two implant crown designs for namely screw-retained and cement-retained. Prostheses utilizing screw retention remain the standard design in most situations for many clinicians while others prefer to cement the restoration which is more of a traditional method. The choice of a screw-retained versus cement-retained crown is a complex and comprehensive decision involving many points of consideration. Advantages cited for screw retention are primarily limited to retrievability. On the other hand, advantages of cement-retained implant restorations include better esthetics, better occlusion, simplicity of fabrication, and reduced cost of components and construction.[3],[5],[18]
The main advantage is retrievability which becomes advantageous in situations such as loosening or fracture of the fastening screws, hygiene, or modification of the prostheses[19]. In areas of limited inter-ridge space, a screw is more effective than cement, because the abutment lacks in height and surface area for the retention of crown. Despite the aforementioned advantages, screw-retained restorations have some short-comings, the important one being lack of versatility in design. Screw-retained implant restorations may have the advantage of predictable retrievability, but they demand precise placement of the implant for optimal location of the screw-access hole. It usually necessitates more complex and expensive lab procedures and also is associated with inherent mechanical complications such as screw loosening and fractures.[20],[21] Moreover, the presence of a screw access opening may interfere with natural occlusal morphology,[3] disrupt the porcelain continuity and result in unstable occlusal contacts.[22],[23] The presence of screw holes on the occlusal surface provides poor esthetics and establishment of an ideal occlusal relationship may not be possible, especially for molars.[24] They also present a screw access opening that can weaken the porcelain around the openings and at the cusp tips, resulting in unstable occlusal contacts.
The rapid acceptance of cemented implant prostheses have been attributed to several factors. They are less costly and utilize fewer prosthetic components. A cemented implant crown is similar to those used in tooth supported fixed prosthesis. It also eliminates the need for a prosthetic screw and the unesthetic occlusal screw access channel through the restoration, thereby improving esthetics, optimizing occlusal loading, and also limiting the incidence of loose screws and associated maintenance.[3] With a loose abutment screw, aggressive attempts to remove the crown may result in damage to the implant inner threads and, subsequently, may compromise the long-term stability of the prosthesis. It is also shown that cement thickness at the occlusal and marginal areas may lead to compromised seating of even well fabricated crowns.[25],[26] the inadequate removal of residual cement in the sulcus can adversely affect the peri-implant soft tissues and long term success of implant itself.
In the particular case, the options of screw-retained and cement-retained implant restorations were assessed. It was decided to opt for a screw-retained implant restoration as the inter-arch space available was limited. The restoration had to be screw-retained for adequate retention. The composite filling helped in concealing the unesthetic screw access hole successfully.
Conclusion
The use of screw-retained crowns has helped to overcome many of the limitations encountered with conventional fixed and removable prostheses. There are advantages and disadvantages to using a screw-retained versus a cement-retained crown.[27],[28],[29] The choice of cementation versus screw retention should be based on the height available for the prosthesis. However, the clinician’s personal preferences also play a role in the selection of type of restoration. There are several arguments for and against each of these two possible methods of fixation, and the controversy still brewing over the choice.
Referernces
1. Adell, R, Lekholm, U, Rockler, B, Brånemark, P, A 15-year study of osseointegrated implants in the treatment of the edentulous jaw. Int J Oral Surg; 2:387–416.
2. Albrektsson T, Dahl E, Enbom L, et al. Osseointegrated oral implants. A Swedish multicenter study of 8139 consecutively inserted Nobelpharma implants. J Periodontol 1988; 59: 287–296.
3. Hebel KS, Gajjar RC. Cement-retained versus screw-retained implant restorations: Achieving optimal occlusion and esthetics in implant dentistry. J Prosthet Dent 1997; 77:28–35.
4. Michalakis KX, Hirayama H, Garefis PD: Cement-retained versus screw-retained implant restorations: a critical review. Int J Maxillofac Implants 2003;18:719-728
5. Chee W, Felton DA, Johnson PF, et al: Cemented versus screw-retained implant prostheses: which is better? Int J Oral Maxillofac Implants 1999;14:137-141
6. Misch CE: Screw-retained versus cement-retained implant-supported prostheses. Prac Periodontics Esthet Dent 1995;7:15-18
7. Sones AD. Complications with osseointegrated implants. J Prosthet Dent 1989; 62:581–585.
8. AdelI R, Lekholm U, Rockier B, Branemark PI. A 15-year study of osseo-integrated implants in the treatment of the edentulous jaw. Int J Oral Surg 1981; 10:387-416.
9. Hansson BO. Success and failure of osseo-integrated implants in the edentulous jaw. Swed Dent J 1977; Supp[ 1:1-101.
10. Cranin NA, Rabkin MF, Garfinkel L. A statistical evaluation of 952 endosteal implants in humans. J Am Dent Assoc 1977; 94:315-20.
11. Adell R, Eriksson B, Lekholm U, Branemark PI, Jemt T. Long-term follow-up study of osseo-integrated implants in the treatment of totally edentulous jaws. Int J Oral Maxillofac Implants 1990; 5:347-59.
12. Zarb GA, Schmitt A. The longitudinal clinical effectiveness of osseo-integrated dental implants: the Toronto study. Part h surgical results. J Prosthet Dent 1990; 63:451-7.
13. Cordioli G, Castagna S, Consolati E. Single tooth implant rehabilitation: A retrospective study of 67 implants. Int J Prosthodont 1994; 7:525–531.
14. Engquist B, Nilson H, Astrand P. Single-tooth replacement by osseo-integrated Brånemark implants. A retrospective study of 82 implants. Clin Oral Implants Res 1995; 6:238–245.
15. Wilson Jr AH, Chan DC. The relationship between convergence and retention of extra-coronal retainers. J Prosthodont 1994; 3:74–8.
16. Covey DA, Kent DKSt, Germain Jr HA, Koka S. Effect of abutment size and luting cement type on the uniaxial retention force of implant supported crowns. J Prosthet Dent 2000; 83:344–8.
17. Kent DK, Koka S, Froeschle ML: Retention of cemented implant-supported restorations. J Prosthodont 1997;6:193-196
18. Keith SE, Miller BH, Woody RD, Higginbottom FL. Marginal discrepancy of screw-retained and cemented metal-ceramic crowns on implant abutments. Int J oral Maxillofac Implants 1999; 14:369-78
19. Chiche GJ, Pinault A. Considerations for fabrication of implant-supported posterior restorations. Int J Prosthodont 1991; 4:37–44.
20. McGlumphy EA, Mendel DA, Holloway JA: Implant screw mechanics. Dent Clin N Am 1998;42:71-89
21. Pietrabissa R, Giono L, Quaglini V, et al: An in vitro study on compensation of mismatch of screw versus cement-retained implant supported fixed prostheses. Clin Oral Impl Res 2000;11:448-457
22. Torrado E, Ercoli C, Al Mardini M, et al: A comparison of the porcelain fracture resistance of screw-retained and cement-retained implant-supported metal–ceramic crowns. J Prosthet Dent 2004;91:532-537
23. Zarone F, Sorrentino R, Traini T, et al: Fracture resistance of implant-supported screw- versus cement-retained porcelain fused to metal single crowns: SEM fractographic analysis. Dent Mater 2007;23:296-301
24. Okeson JP. Management of Temporo-mandibular Disorders and Occlusion, ed 2. St Louis: Mosby, 1989:59–86.
25. McLean JW, von Fraunhofer JA: The estimation of cement film thickness by an in vivo technique. Br Dent J 1971;131:107-111
26. Dimashkieh MR, Davies EH, von Fraunhofer JA: Measurement of the cement film thickness beneath
27. Goodacre CJ, Bernal GB, Rungcharassaeng K. Clinical complication with implants and implant prostheses. J Prosthet Dent. 2003; 90:121–32.
28. Weber HP, Kim DM, Ng MW, et al. Peri-implant soft-tissue health surrounding cement- and screw-retained implant restorations: a multi-center, three year prospective study. Clin Oral Implants Res. 2006; 17:375–79.
29. Sheets JL, Wilcox C, Wilwerding T. Cement selection for cement-retained crown technique with dental implants. J Prosthodont. 2008; 17:92–96.\
|